China's Barefoot Doctors
Health care by and for the people
BOTH the popular press and various medical journals in recent years have carried reports on the health delivery rendered by nearly one million barefoot doctors in China. In one sense, the functions carried out by the barefoot doctors could be equated with the roles of Medex nurse-practitioners, midwives, and feld-schers that have developed in this country and elsewhere. Barefoot doctors are generally recruited from the ranks of the peasants to carry out simple medical procedures among commune residents. (The term "barefoot" is symbolic of the close tie these paramedics have with the once shoe-less peasants.) In addition to working in rural areas, barefoot doctors are also present in factories and in urban neighborhoods, although other terms are used for them: "worker-doctors" in factories and "red guard doctors" in the neighborhoods.
How barefoot doctors reach this stage functioning is very different. For one thing, impetus was provided by the June 26, 1965, directive from Chairman Mao which essentially stated that health delivery must be implemented in rural areas. However. barefoot doctors just did not suddenly emerge. In the 1930s, Dr. Norman Bethune, a Canadian physician who served with the Communist Eighth Route Army started to train peasants to carry out some paramedical duties. The number began to grow in the 1950s, and the 1965 directive hastened this process.
There has also been a conscious effort to utilize all available training resources in local areas so that the barefoot doctors will recognize and serve the needs of the people in those areas. For example, at the Hsich'ang-an Street Neighborhood, Peking, we talked with a 49-year-old woman barefoot doctor who was barely literate, She was trained for three months to carry out some minimal first aid functions. A physician from Peking Hospital No. 2 was there four days a week to supervise her activities. The physician mentioned that now this barefoot doctor is encouraged to diagnose patient illnesses (the physician provides a backup diagnosis) and to seek additional training at nearby medical schools and hospitals. At the other extreme. we met barefoot doctors at the August 1 Commune in Shen Yang who received one or two years of formal training at a school of public health in the city. These barefoot doctors also carry out medical routines more independently. We talked with some who even performed vasectomies and minor surgery.
The coordination between various health groups allows the barefoot doctors to have the support of larger facilities. The August 1 Commune, with 21,000 people, for instance, has 26 barefoot doctors (8 women and 18 men, all young) who work in the 15 brigades. At the commune level, there is a small 30-bed hospital with 38 health personnel, including 12 physicians, 10 nurses, 4 barefoot doctors, and other technical staff. At the city level, there are two large hospitals; the one we visited, which concentrated on Chinese traditional medicine, has 400 beds and 1,500 staff personnel, many of whom are with the Liaoning School of Chinese Medicine. The other hospital is affiliated with a Western medical school. This commune started with six barefoot doctors in 1965, two more were added in 1970, another five in 1971, and 12 more in 1972-1973. They are part of the 38,000 barefoot doctors in Liaoning Province, with a population of 34 million, who work in 1,330 commune and urban locations, backed by 6,100 Chinese medicine physicians, 15,000 university graduated physicians, 14,000 physicians with less than university training,* and 26,000 nurses Their patients who need such care can enter hospitals with a total of 94,000 beds, as compared with 8,900 beds available in 1949.
The training given to barefoot doctors must be seen within the total context of training of all health personnel. After years of hiatus, all physicians now receive a combination of Chinese and Western medical training. Herbal medicine, acupuncture treatments, and other Chinese techniques are taught along with Western medicines. Thus, a recent InstructionalManual for the Barefoot Doctors (with at least two regional editions describing ways of treating illnesses indigenous to the areas) contains 131 pages devoted to herbal medicine and another 30 pages on acupuncture, besides 430 pages on how to diagnose and treat common ailments. In addition, physicians in China have made remarkable medical advances which have caught the eyes of Western health observers: flexible splints for fractures, treatment for severe burn cases, reimplantation of severed limbs and extremities, dental extraction without the use of local anesthetics, cauterization of tonsils, acupuncture as analgesia, just to name a few.
In the area of preventive and public health, the Chinese have also accomplished a great deal, although here we were frustrated in not being able to obtain consistent data on a few standard statistics that reflect public health advances. The lack of statistics has also hampered others who have visited China recently. Nevertheless, at the various places we visited, we did get some indication that birth and death rates are down. Some rates seem almost too low. We had no data for infant mortality which is a good indication of public health advances. The few statistics we were able to get on crude birth and death rates (per thousand) for 1972 follow on the next page.
Birth rates are down due to intensive periodic mass campaigns on family planning which stress the following: (1) late marriage, for men ideally around age 27 and for women around 24; (2) two children per family, spaced five years apart; (3) use of contraceptive measures, including intrauterine devices, pills, vasectomies, and even, in a number of situations, abortions; and (4) no pre-marital sex. On this last point, we should mention that young people seem to have adopted a highly moralistic sex code. Whenever we encountered groups of young people, we would ask how they are able to accomplish this. The answer was, "We do a lot of activities together and we have group companionship." At the Liaoning School of Chinese Medicine, where we interviewed 12 former barefoot doctors who are now receiving their medical training, we inquired whether they feel our Western colleagues would actually believe that there is little or no pre-marital sex going on. They all had a hearty laugh and said, "Well, whether your friends believe us, this is actually what is going on." Whether or not this is true, the fact that venereal disease, from all reports, is practically eradicated is a good indication that "loose" sex behavior is now practically minimized.
The periodic mass campaigns also extend into other areas of public health, such as ridding the country of the four pests flies, mosquitoes, rats, and lice. Certainly the children we met seemed robust and healthy (they receive every conceivable immunization from birth to 18 months) and their scalps no longer showed the tell-tale splotches of bites from lice. They also seemed to have sufficient food, clothing and shelter, although cities are still teeming with people. Communicable disease, such as cholera and yellow fever, are controlled to the extent that some of the medical schools feel that minimal training is needed in these areas. Some regions still have schistosomiasis, an illness carried by snails, but this is also coming under control. In one commune we were told that when a campaign was mounted against the .snail parasites, feces of humans and animals were carefully scrutinized. Diseased traces were covered in airtight vats for a number of months until the parasites were eliminated before the "night soil" was used as fertilizer. The distance between wells and latrines is also carefully measured. In general, preventive health measures are systematically being carried out.
As we saw all these advances in the health area, one question kept running through our minds, "How is China able to bring this about?" Although not political analysts, we could hazard a few speculations. Perhaps the best way to understand why some dramatic changes have occurred in the health area is to recognize that China is now a tightly organized country. Administratively, urban areas are divided into a series of local governments, starting with the central government in Peking, down to the provincial level municipalities, districts (each of which may cover 250,000-500,000 people), street committees and neighborhood committees. Similarly, rural areas are localized to communes (with approximately 20,000-50,000 people) and further divided into brigades and prediction teams. Urban street committees an. communes have their own party and revolutionary committees which are essentially policy-making bodies. Factories, schools, and other institutions have similar party and revolutionary committees. For instance, August 1 Commune in Shen Yang, where we spent 4 days, has 15 brigades further subdivided into 73 production teams, the total consisting of 20,853 people.
On some issues, the commune residents are able to come to an autonomous decision on the way they want things carried out. For instance, barefoot doctors are paid by their commune, the amount depending on the annual income of the entire commune. Health insurance implementation is also a local matter. Many of the commmunes and neighborhood areas now have cooperative health insurance plans for individuals. The amount which each individual pays varies according to the fiscal solvency of that commune. In one commune we visited, when the cooperative health plan was drawn up, it was estimated that the amount would be equivalent to $1.50 per person, with half the amount paid by the commune. However, after a year's experience, that commune found that too much money was being collected. For the following year, the amount was reduced to $1.00 per person.
In addition to paying the barefoot doctors, some communes also use health insurance and registration fees to finance equipment for the hospital. Since 1969, when a cooperative health plan campaign started in Liaoning Province, 95 per cent of the 16,000 brigades in 1,330 communes have adopted the plan. Sixty per cent of these brigades have well equipped clinics. The remaining brigades which do not have cooperative health plans may be either too poor or they are so well off that members can afford to pay for their own health needs.
Aside from the issue of centralization and decentralization, certain traditional blocks have been removed from Chinese health training. The philosophy of integrating theory and practice pervades all areas of higher education. As a result, the idea of an elite medical profession now takes second place to "serving the people." License requirements and formal educational requirements are played down so that a maximum number of people can receive the necessary health skills. "Ideological correctness" also takes precedence over other requirements when young persons are selected by their peers to take further training. We have no idea how this will ultimately affect the quality of health care in China. However, one thing became clear to us: Where no health personnel or services were available to large numbers of people before 1949, at least most Chinese have minimal care now. This surely represents a great leap forward for the people.
*Since the cultural revolution (1965-1968) many middle school graduates can enter medical schools after have worked three years.
Crude Total CrudeLocations Birth Rate Population Death Rate Canton Health Department 19.7 5.2 3,000,000 Canton Family Planning Committee 26* 5 3,000,000 July 1 Commune (Shanghai) 13 8 17,000 Nan-Ying Commune (Shanghai) 14 4 27,000 Tsao-yang Village (Shanghai) 5.28 3.68 70,000 Evergreen Commune (Hangchow) 16 2 22,000 Mei-chai wu Commune (Hangchow) 19 5.5-6.0 10,500 A Street Committee (Hangchow) 8.47 5.8 2,700 Liaoning Province 24 6 34,000,000
*Possibly, the Canton Family Planning Committee gave statistics on another population. This is a good example of inconsistent data.
Not a campaign against running dog imperialists, these signs exhort Chinese to battle against disease-carrying pests.
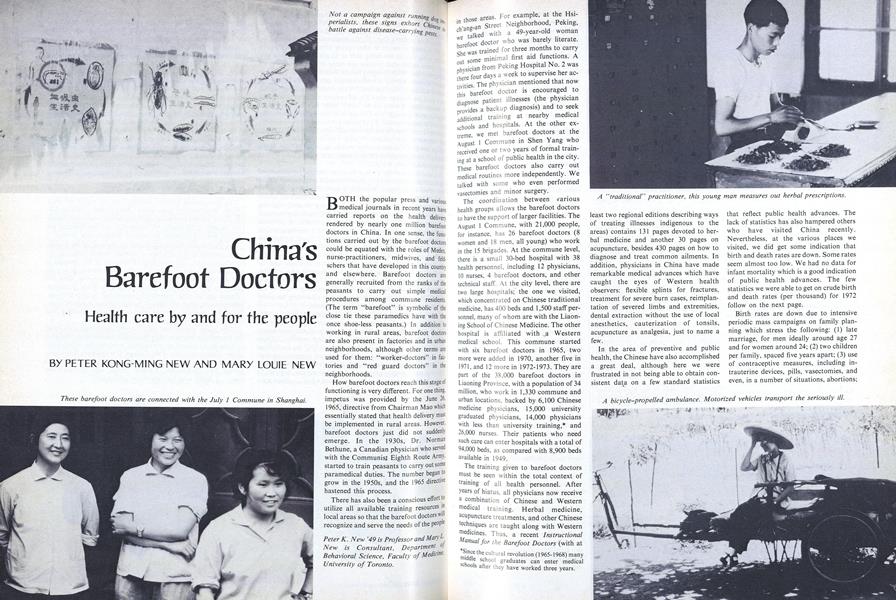
A "traditional" practitioner, this young man measures out herbal prescriptions.
Students at Liaoning School discuss the salutary effects of "group companionship."
A barefoot doctor, dressed inegalitarian costume of the peasants. administers health care to fieldworkers.
Peter New, who emigrated as a boy from Shanghai with his family (his father was aHarvard-trained physician), strikes a tourist's pose at the Great Wall last summer.
Peter K. New '49 is Professor and Mary L.New is Consultant, Department ofBehavioral Science, Faculty of MedicineUniversity of Toronto.