Life in High Places
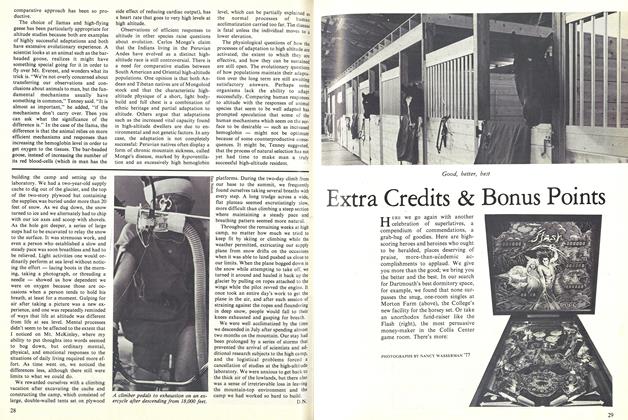
Bar-headed geese, during the course of their migration, fly over the Himalayas at altitudes as high as 30,000 feet. Reinhold Messner one of the world's most competent and ambitious mountaineers, has climbed to the summit of Mt. Everest without the aid of an artificial oxygen supply. Many generations of men, women, and children have lived productive lives in high-altitude communities such as the one at Ticlio, Peru, at 16,000 feet.
But adaptability has limits. There has been no permanent human habitation higher than 18,000 feet. Natives of the Andes sometimes lose their acclimatization to altitude and are forced to live near sea level to survive. Although some animal species-the llama, for example-thrive at high altitudes, others-such as commercial breeds of cattle-don't adapt well at all. Individuals who reside near sea level are likely to experience the unpleasant sensations of acute mountain sickness-headache, nausea, listlessness, and insomnia after making a rapid ascent to elevations above 9,000 or 10,000 feet. Scores of people-many of them healthy and vigorous climbers, skiers, and mountain trekkers-die every year of causes related to altitude, particularly a malady known as high-altitude pulmonary edema in which the victim literally drowns in fluid accumulated in the lungs. Some individuals never experience altitude-related illness, others can't ascend very far without feeling sick, and still others react well on one occasion but poorly on another.
Hypoxia, or oxygen deficiency, is the main problem for life at high altitude. Although the percentage of oxygen in the atmosphere remains the same at high altitudes as at sea level, the oxygen pressure is reduced. As altitude increases, the barometric pressure decreases, reducing the pressure of oxygen in the air. The reduced oxygen pressure makes it more difficult to move oxygen to the cells of the body. At 18,000 feet, for example, the partial pressure of oxygen is about half of what it is at sea level. The body has to compensate for that deficiency by moving twice the volume of air as it would at sea level in order to obtain the same number of oxygen molecules.
Because the body's functions are so absolutely dependent on maintaining a critical level of oxygen saturation, the crucial problem at high altitude is getting enough oxygen from the environment into the lungs, into the blood stream, and finally down to the mitochondrial level of the cell where energy is generated. The process by which the body succeeds in preventing the oxygen-deficient condition of hypoxia at high altitude is called acclimatization. The important questions for scientists interested in altitude are how the physiological processes of acclimatization are activated, the extent to which they are effective, and how they are sustained. Scientists are also asking how human or animal populations maintain their'adaptation to altitude, and wondering what evolutionary processes are at work.
High-altitude physiology has been a serious interest at the Dartmouth Medical School for over 25 years, and much of that research has involved Dr. S. Marsh Tenney '44, Nathan Smith Professor of Medicine, former dean of the Medical School, and chairman of the Physiology Department since 1956. Work in this field, carried out mostly in the laboratory by using pressure chambers to simulate the high-altitude environment, also takes researchers to mountain tops. Since the early 19505, Tenney and his colleagues have collaborated on a long list of research projects-ranging from measurements of respiratory mechanisms at high altitude, to studies of the interaction of chemical stimuli affecting respiration, to investigation of influences by the cortical region of the brain on the control of breathing. Studies of this sort are an important adjunct to a general understanding of cardiovascular and respiratory physiology, Tenney said during a recent conversation about his interest in high-altitude research. Some of the most serious problems in those broader areas of physiology have to do with oxygen transport and the adequate oxygenation of tissues, and it is enlightening for a medical scientist to see how problems with oxygen arise and are dealt with by healthy people in oxygen-deprived environments. Not incidentally, high-altitude research can provide an attractive combination of scientific work and adventure in some of the most dramatically scenic parts of the world.
The problems of mountain sickness had been described as early as the 17th century by Spanish missionaries in the Andes, and there also is historical evidence that the Incas had long been aware of health problems peculiar to their communities high in the mountains. Serious scientific interest in high-altitude physiology originated about a century ago, Tenney recounted, as the result of problems related to balloon ascents. In the late 1800's, four Frenchmen involved in a well-known and disastrous ascent somehow lost control of their balloon. As the craft went higher, they lost their ability to deal with the situation. Three of the crew members died, and scientists wondered if the victims' physiological problems were a consequence of the reduction in the barometric pressure as the balloon ascended, or if their difficulties were more directly a result of the diminution of the partial pressure of oxygen at high altitude. Research done by the French physiologist Paul Bert showed that oxygen was the issue and.stimulated a lively series of studies, conducted mostly in the Alps by European scientists, concerned with exploring some of the problems and consequences of low oxygen pressure and supply.
During the early part of this century, Tenney explained, the field came to take on two general patterns. First, there was the use of the high-altitude environment as a tactic or tool for exploring the problems of hypoxia, which are present in a wide variety of diseases. The second theme was a much broader interest in the general biology of high altitudes-a concern with the investigation of characteristics of entire populations, both plant and animal, that led to questions about evolution. In the Peruvian Andes, where large human populations live at high altitudes, this area of study was pursued with particular vigor, Tenney noted. The father of this second branch of research, Carlos Monge did a series of physical anthropological studies of natives in the Andes-measurements of chest size, for example-and proposed that they had evolved as a distinct race of high-altitude people.
Studies more specifically focused on physiology were performed primarily by American, British, and German researchers who were interested in the fundamental nature of respiratory responses and mechanisms. World War II and the practical importance of altitude-related problems in aviation medicine and technology gave a boost to the science. In Peru, the physiologist Alberto Hurtado, a pupil of Carlos Monge, stimulated renewed interest in the high-altitude Indian population as the result of research carried out at the laboratory he established at almost 15,000 feet in the mining town of Morococha
Tenney cited the question of how breathing is controlled as an example of a basic physiological problem that has been profitably investigated at high altitude. It has also been a subject that he and his colleagues at Dartmouth have come Back to repeatedly. The mechanisms at work in the control of breathing-their development and changes-"have been a dominant and continuous thread here, a sustaining component of our research," Tenney said. In the 1950s and sixties, John Remmers '59, John Mithoefer Kenneth Falchuk '62, and Tom Lamb-doctors who subsequently went on to departments of medicine and physiology at other medical schools-collaborated with Tenney on a variety of projects concerned with the control of breathing and ventilatory acclimatization at high altitude. Tenney and Lo Chang Ou an assistant professor of physiology at Dartmouth, have investigated central nervous mechanisms affecting breathing at altitude, and John G. Brooks, a former Dartmouth medical student, and Craig P. Black, a research fellow, contributed to comparative studies of ventilatory function in different animal species.
One reason why the subject of the control of breathing has been so tantalizing, Tenney explained, is that breathing is the only significant body function subject to both voluntary and involuntary control. The amount of oxygen required by the body is exactly matched by the amount of oxygen consumed, so the partial pressure of oxygen in the body remains almost constant. This accomplishment is remarkable, he added, because metabolic requirements fluctuate depending on activity. Despite the special stresses that occur when the oxygen supply is limited, breathing is always regulated to respond in proportion to the body's demand.
The most important way the body responds to high altitude is by reducing the difference between the pressure of oxygen in the air and the pressure of oxygen at the level of the cell. A certain amount of pressure is needed to transfer oxygen to the blood. At 18,000 feet, for example, where the partial pressure of oxygen is about half that at sea level, the body is able to reduce the existing pressure gradient largely by increasing the pressure in the air pockets of the lungs through hyperventilation. This response (called the hypoxic ventilatory response) is prompted when the peripheral chemoreceptors (oxygen-sensitive nerve endings that play a role in the control of breathing) are stimulated by hypoxia. During hyperventilation, however, the body is blowing off carbon dioxide, which has the consequence of increasing the alkalinity of the system and puts a damper on ventila tion. The body tries to keep the respiratory system in balance by eliminating excess bicarbonate through the kidneys. This chain of responses occurs to maintain an adequate level of oxygenation, and the process is regulated in part by the chemical influence of the acid-base balance in the body.
Tenney pointed out that in the mid-1950s there was a general recognition that changes in the cerebrospinal fluid (the fluid that bathes the brain) also play an important part in regulating this system. At Dartmouth and elsewhere, questions about how mechanisms apart from the acid-base balance are related to ventilation led to a whole range of new studies of how breathing is controlled at high altitude. Scientists wondered how the reactivity of the cerebrospinal fluid does, in fact, stimulate breathing, how the fluid's composition is determined, and what kind of equilibrium it has with the composition of the blood and the rate of blood flow. In general, though, what happens during human acclimatization is that a balance is achieved between the various excitatory and inhibitory influences on ventilation. Over the first few days of exposure to altitude, the ventilatory rate gradually increases as a consequence of a readjustment in the acid-base balance. Over time, the sensitivity to hypoxia is attenuated, and in long-term high-altitude dwellers the hypoxic ventilatory response is lost almost completely. As the body acclimatizes, the transport of oxygen from the lungs to the tissues may be slightly helped by an increase in the rate of oxygen diffusion from the alveioli into the blood. The cardiac output also increases, and immediately upon exposure to altitude the body begins manufacturing more red blood cells to increase the blood's oxygen-carrying capacity. Finally, the capillary density increases in order to aid diffusion of oxygen from the capillaries to the cells. Comparative physiological studies with other species have shown that not all these adaptive responses in humans are as beneficial as they first appear, Tenney noted.
Scientific questions arise concerning each step in the process of acclimatization, Tenney observed, and at Dartmouth high-altitude research has proceeded in two main directions. The first area of investigation has been concerned with the control of breathing; the second has been a consideration of the general question of how, in the face of a diminished oxygen supply, an organism as a whole manages to adjust its regulatory systems to make sure enough oxygen is distributed. The origin of pulmonary hypertension at high altitude is a specific question currently under investigation at Dartmouth. Tenney and Susan Snow, a medical student, have been looking at the change in pulmonaryartery pressure in response to hypoxia. Pulmonary arterial circulation constricts at altitude, Tenney explained, which raises pulmonary-artery blood pressure, and as a consequence the right side of the heart has to work harder. "It's hard to think of that as serving a useful purpose," he noted. Ron Jones, a research fellow, and Tenney have also been looking at water balance in the body and at how hypoxia inhibits the urge to drink-an aspect of high-altitude life that mountaineers must take pains to overcome in order to avoid dehydration. In addition to their studies of the central nervous mechanisms affecting ventilation, Professor Ou and Tenney have investigated biochemical and metabolic factors in acclimatization. The question of failures in the process of acclimatization is a line of research Ou has continued independently.
"We have suspected a strong contribution to the control of breathing from the central nervous system, independent of the acid-base balance," Tenney said of one series of recent studies. "In the early stages of hypoxic exposure, the level of ventilation is higher than would be predicted because of the chemical influence. We suspect a primitive back-up system in the brain which provokes a generalized reaction which arouses ventilation." This would be accomplished, he explained, through "afferent pathways between the chemoreceptors and an arousal area of the brain very much affected by hypoxia." (It is interesting to note, Tenney observed, that there is a great deal of nervous arousal commonly experienced at altitude-insomnia, for example, as well as general irritability and restlessness.) Work in this area has also led Tenney and his colleagues to suspect an inhibitory influence from the cortex to hold the arousal features affecting ventilation in check a new and still unproved notion.
Expanding interest in mountaineering and the recent increase in the number of people exposed to high altitudes because of participation in mountain tours, treks, helicopter skiing vacations, and the like, has stimulated scientists to ask some practical and pressing questions about altitude illness, Tenney observed. He also commented that "part of the fun of working with high altitudes" is thinking about the conditions and mechanisms that have counterparts in disease at sea level. "We've seen all along the way that lessons at high altitude are applicable to clinical situations," he added, "because the most threatening situations in a very large number of diseases-certainly all the respiratory illnesses-have to do with problems of oxygen supply." The problems of hypoxia create serious handicaps for individuals who are already sick, and it can be productive to view those problems against the healthy high-altitude dweller who is able to make satisfactory adjustments to hypoxia.
The emphasis of high-altitude studies at Dartmouth has shifted gradually from humans to animals for a variety of reasons. It used to be, Tenney said, that animal experimentation was limited because the ordinary logistical problems of high-altitude expeditions to mountainous areas, already complicated by taking along scientific instruments, were compounded even further by taking animals. In the early 19705, however, with the construction of new Medical School facilities, the Physiology Department obtained a large pressure chamber for simulating the high-altitude environment in the laboratory, which made animal experimentation much easier. Questions that can be investigated in an animal in a straightforward manner might require roundabout, impractical, or unethical procedures in man. One of the main reasons for using a wide variety of species for physiological research at Dartmouth, however, is that the exploitation of the comparative approach has been so productive.
The choice of llamas and high-flying geese has been particularly appropriate for altitude studies because both are examples of highly successful adaptations and both have extensive evolutionary experience. A scientist looks at an animal such as the barheaded goose, realizes it might have something special going for it in order to fly over Mt. Everest, and wonders what its trick is. "We're not overly concerned about transferring our observations and conclusions about animals to man, but the fundamental mechanisms usually have something in common," Tenney said. "It is almost as important," he added, "if the mechanisms don't carry over. Then you can ask what the significance of the difference is." In the case of the llama, the difference is that the animal relies on more efficient mechanisms and responses than increasing the hemoglobin level in order to get oxygen to the tissues. The bar-headed goose, instead of increasing the number of its red blood-cells (which in man has the side effect of reducing cardiac output), has a heart rate that goes to very high levels at high altitude.
Observations of efficient responses to altitude in other species raise questions about evolution. Carlos Monge's claim that the Indians living in the Peruvian Andes have evolved as a distinct highaltitude race is still controversial. There is a need for comparative studies between South American and Oriental high-altitude populations. One opinion is that both Andean and Tibetan natives are of Mongoloid stock and that the characteristic highaltitude physique of a short, light bodybuild and full chest is a combination of ethnic heritage and partial adaptation to altitude. Others argue that adaptations such as the increased vital capacity found in high-altitude dwellers are due to environmental and not genetic factors. In any case, the adaptation is not completely successful: Peruvian natives often display a form of chronic mountain sickness, called Monge's disease, marked by hypoventilation and an excessively high hemoglobin level, which can be partially explained as the normal processes of human acclimatization carried too far. The disease is fatal unless the individual moves to a lower elevation.
The physiological questions of how the processes of adaptation to high altitude are activated, the extent to which they are effective, and how they can be sustained are still open. The evolutionary questions of how populations maintain their adaptation over the long term are still awaiting satisfactory answers. Perhaps some organisms lack the ability to adapt successfully. Comparing human responses to altitude with the responses of animal species that seem to be well adapted has prompted speculation that some of the human mechanisms which seem on the surface to be desirable such as increased hemoglobin-might not be optimum because of some counterproductive consequences. It might be, Tenney suggested, that the process of natural selection has not yet had time to make man a truly successful high-altitude resident.
Dr. S. Marsh Tenney '44 uses a low-pressure chamber for high-altitude research.