Is There a Robot In the House?
A doctor with an eye on the future invites students to invent the health care of tomorrow.
A doctor with an eye on the future invites students to invent the health care of tomorrow.
A doctor with an eye on the future invites students to invent the health care of tomorrow.
PICK UP ANY NEWSPAPER and you'll read about advances in gene mapping and drug therapies that will cure a multitude of human ailments in the future. But in a large lecture hall at the Thayer School of Engineering, Dr. Joseph Rosen, a plastic surgeon at DartmouthHitchcock Medical Center (DHMC), teaches a class that focuses on another part of medical innovation: assembling the nuts and bolts—and bits and bytes- of the technologies that will revolutionize health care in the coming decades. While biochemists struggle to create new medicinal compounds, doctors with an engineering bent are dreaming up—and building—such technical wonders as computer chips that will renew function to damaged nerves and robotic hands that will allow doctors to perform longdistance surgery.
The road to the future, explains Rosen, is paved with the imaginations of an endless network of people—including Dartmouth undergraduates. Four years ago he developed "Healthcare and Technology in the 21st Century," an unusual engineering course he teaches to rev the minds of those who will drive the medical advances of the future.
Students quickly find that they are not just along for the ride. Whether they're future doctors, budding engineers or English majors satisfying a science requirement, Rosen invites them to brainstorm solutions to a wide range of medical challenges, such as how to improve life for amputees by making prosthetic limbs easier to use. Despite the size of the class—enrollments range from 60 to 90 students—Rosen creates a thinktank atmosphere of participation and collegiality, key elements of his formula for innovation and venturing out of the box. He gives students ample time to ask questions during PowerPoint-studded lectures. He updates them on the latest medical advances via a 600-page reader assembled for the course and through postings on the class Web site. He encourages students to unleash their creativity when they write papers—after all, he says, any one of them could come up with the next great medical innovation. He notifies students of internship opportunities at Dartmouth and elsewhere. Each year he even hires five or six undergraduates to serve as teaching assistants for the course.
Rosen introduces students to three broad areas of medical care: repairing damaged limbs and tissues; using imaging techniques such as virtual reality to view the body in increasingly sophisticated ways; and developing the computer and robotic technologies that will allow what he calls "telemedical" links between doctors and remote patients. Having worked in all these areas, Rosen could deliver all the lectures himself. But he chooses to enlist guest speakers for at least half of the presentations. That way, "students get different perspectives. They learn there's more than one definition of anything," he says.
Some of the guests, such as artificial intelligence pioneer Marvin Minsky, have invented new fields. Others, including many of Rosens colleagues at DHMC, give students a direct look at how real doctors use a variety of medical toolsand how the devices could be improved.
For example, in one presentation a gastroenterologist passes around a couple of endoscopes—long, thin tubes that allow him to examine the digestive track. One scope is stiff and unyielding. "What are its drawbacks?" he asks. Students point out its limited range of vision. The other scope is flexible enough to thread through a colon to look for signs of disease. "This is the ultimate video gamechasing polyps, ulcers and cancers," the doctor says. Then he tells the class about his work to develop a tool that would go beyond the capabilities of even the most sophisticated endoscopes—a small robotic device that would propel itself through the digestive track to diagnose and fix problems.
In another class a cardiologist describes how a new three-dimensional computer model reveals that a beating heart twists in ways that doctors could not easily visualize before. Excessive twisting may indicate an impending stroke. The new model will allow doctors to intervene before irreparable damage is done.
In other lectures students learn how imaging techniques such as MRIs are opening up new views of the body. "You don't hear the term exploratory surgery' any more," says one of the guest speakers.
Students hear about the need for surgeons to practice on computer models—virtual patients—instead of real people. They see how surgeons peering at lifelike 3-D images of a patient will go through the motions of surgery—literally—while remote sterile robotic hands reproduce those precise movements, from incisions to sutures, on the patient, who might be on a distant battlefield or one day maybe even on Mars. Students learn, too, about the astounding world of nanotechnology—molecular machines capable of rearranging atoms to cure diseases and cellular damage. "It sounds like science fiction," admits the nanotechnology lecturer, DHMC anesthesiologist Christopher Wiley '74. "but a hundred years ago, howwould computers, TV, MRI, space flight and biotechnology have sounded?"
Rosens commitment to bringing students into contact with such an array of thinkers continually underscores the role that networking plays in pushing ideas forward. He also makes that point with anecdotes of his own. For example, Rosen tells the class how he started work on an implantable nerve chip that he hopes will one day allow severed nerves to function again. "I was sitting around eating pizza and reading the manual for a laser disc player in 1983," he says. By the end of his meal a new idea had taken shape in Rosens mind: If the laser disc player could read spots three microns across- about the size of a nerve—lasers should be capable of drilling nerve-sized holes in a microchip. To translate the idea into new technology, he started to network. "I asked around to find someone who could do the drilling. Eventually I met someone who could," he says. "If you keep asking how to solve technical problems, eventually someone knows how."
Rosen, who is still trying to make his nerve chips work, uses the technical complexity of the project to highlight another side of innovation: that new ideas involve risk. "I try to emphasize that failure is okay. If you're trying something hard you're going to have failures," he says. But where there's a willingness to take new approaches, he insists, complicated technologies such as nerve chips will eventually succeed.
Today's students already have a huge technological advantage, according to guest lecturer Richard Satava, a U.S. Army doctor working on remotesurgery methods. "Dr. Rosen and I are dinosaurs," he tells the class. "We were born in the industrial age, in two dimensions. You are in the digital, three- dimensional age. You are the future. Usually the younger the generation, the better the ideas. You owe it to me to tell me where the future is going."
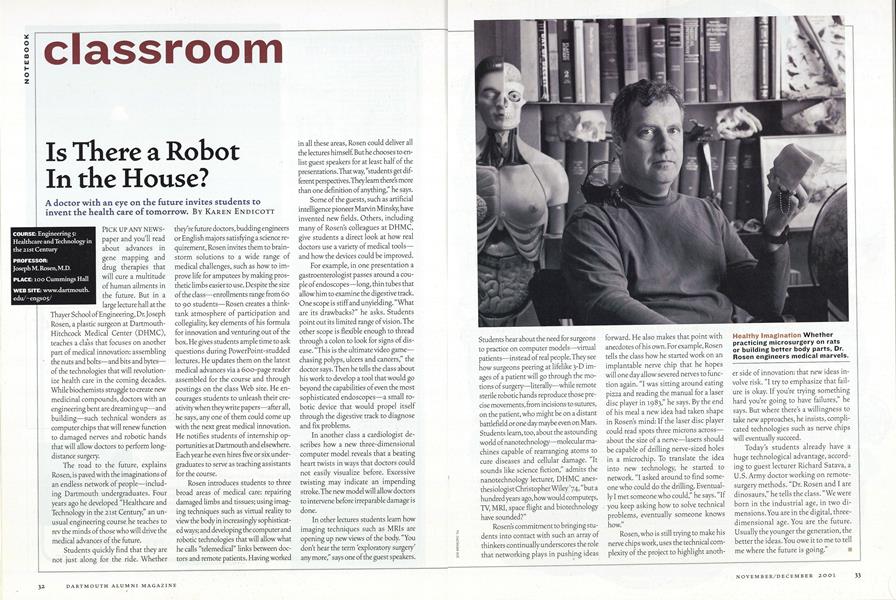
Healthy Imagination Whetherpracticing microsurgery on ratsor building better body parts, Dr.Rosen engineers medical marvels
COURSE: Engineering 5: Healthcare and Technology in the 21st Century PROFESSOR: Joseph M. Rosen, M.D. PLACE: 100 Cummings Hall WEB SITE: www.dartmouth.edu/~engs05/
More From This Issue
-
 Feature
FeatureComing of Age in Hanover
November | December 2001 -
 Cover Story
Cover StoryHow Does Our Garden Grow?
November | December 2001 -
 Big Picture
Big PictureSeptember 11, 2001
November | December 2001 -
 Alumni Opinion
Alumni OpinionThe Ex-Wives Club
November | December 2001 -
 Article
ArticleSeen & Heard
November | December 2001 -
 Class Notes
Class Notes1994
November | December 2001